
ผลลัพธ์ของการตรวจสอบการสั่งยาและให้ข้อเสนอแนะกลับในการสั่งใช้ยา meropenem ในหอผู้ป่วยอายุรกรรม โรงพยาบาลทั่วไป
คำสำคัญ:
การตรวจสอบการสั่งยาและให้ข้อเสนอแนะกลับ, meropenem, de-escalationบทคัดย่อ
ความเป็นมา: Antimicrobial stewardship program (ASP) เป็นกระบวนการส่งเสริมการใช้ยาต้านจุลชีพอย่างเหมาะสม โดยโรงพยาบาลพระพุทธบาทพบปัญหาเชื้อดื้อยาเพิ่มขึ้น ส่งผลให้มีการปรับมาใช้ meropenem มากขึ้น แต่บางกรณีอาจมีการใช้ยาไม่เหมาะสม จึงนำกระบวนการการตรวจสอบการสั่งใช้ยาและให้ข้อเสนอแนะกลับ (prospective audit and feedback; PAF) ซึ่งเป็นกระบวนการหลักของ ASP มาใช้
วัตถุประสงค์: เพื่อเปรียบเทียบร้อยละของการ de-escalation จำนวนวันที่ใช้ยาปฏิชีวนะ ผลลัพธ์การรักษาที่ดีขึ้น ณ วันที่ 3, 5 และ 7 และอัตราการตายที่ 30 วัน ของผู้ป่วยที่ได้รับ meropenem ในการรักษาแบบ empirical therapy ตามแบบแผนปกติ และกลุ่มที่ได้รับกระบวนการ PAF
วิธีวิจัย: การศึกษาย้อนหลังเชิงพรรณนา เปรียบเทียบกลุ่มที่ได้รับการรักษาตามแบบแผนปกติ ระหว่างวันที่ 1 ธันวาคม พ.ศ. 2565 ถึง 31 พฤษภาคม พ.ศ. 2566 และกลุ่มที่ได้รับการรักษาตามกระบวนการ PAF ระหว่างวันที่ 1 มิถุนายน พ.ศ. 2566 ถึง 30 พฤศจิกายน พ.ศ. 2566 กลุ่มตัวอย่างผู้ป่วยที่เข้าเกณฑ์การศึกษาจำนวน 80 ราย แบ่งเป็นกลุ่มละ 40 ราย
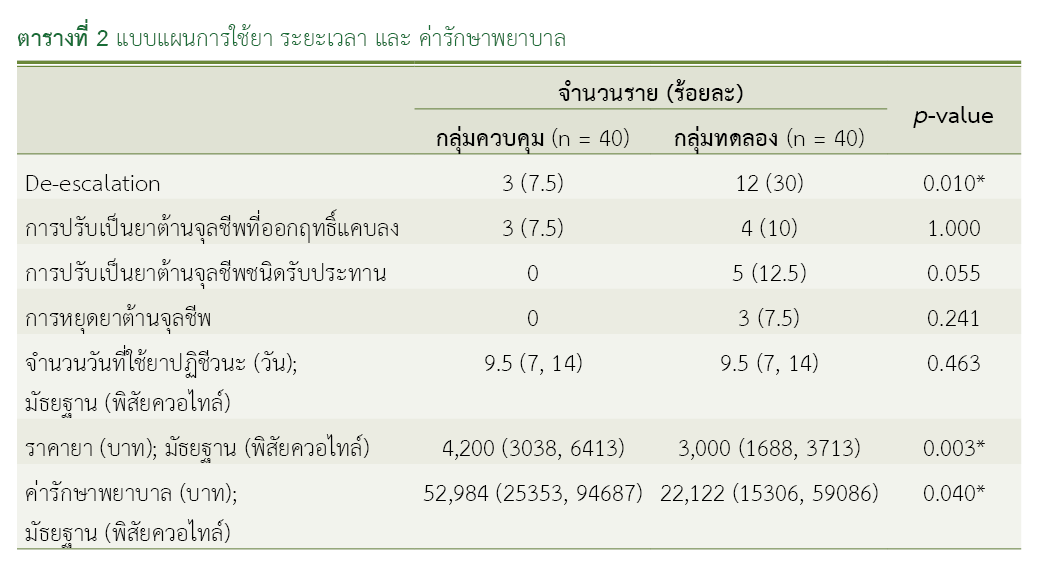
ผลการวิจัย: กลุ่มที่ได้รับการรักษาตามแบบแผนปกติ และกลุ่มที่ได้รับการรักษาตามกระบวนการ PAF พบร้อยละของการ de-escalation เท่ากับ 7.5 และ 30 ตามลำดับ แตกต่างอย่างมีนัยสำคัญทางสถิติ (p-value = 0.01) เมื่อพิจารณาผลลัพธ์การรักษาที่ดีขึ้นในวันที่ 3 พบกลุ่มที่ได้รับการรักษาตามกระบวนการ PAF สูงกว่ากลุ่มที่ได้รับการรักษาตามแบบแผนปกติอย่างมีนัยสำคัญทางสถิติ (p-value = 0.014) แต่ผลลัพธ์การรักษาที่ดีขึ้นในวันที่ 5 และ 7 จำนวนวันที่ใช้ยาปฏิชีวนะ และอัตราการตายที่ 30 วัน ไม่แตกต่างกันอย่างมีนัยสำคัญทางสถิติ
สรุปผล: การตรวจสอบการสั่งใช้ยาและให้ข้อเสนอแนะกลับช่วยเพิ่มการ de-escalation ส่งผลให้เกิดการใช้ meropenem อย่างเหมาะสม
เอกสารอ้างอิง
ศูนย์เฝ้าระวังเชื้อดื้อยาต้านจุลชีพแห่งชาติ (NARST). สถานการณ์เชื้อดื้อยาต้านจุลชีพ ปี 2000-2020(12M) [อินเทอร์เน็ต]. นนทบุรี: ศูนย์เฝ้าระวังเชื้อดื้อยาต้านจุลชีพแห่งชาติ (NARST) สถาบันวิจัยวิทยาศาสตร์สาธารณสุข กรมวิทยาศาสตร์การแพทย์; 2565 [สืบค้นเมื่อ 1 ม.ค. 2566]. สืบค้นจาก: http://narst.dmsc.moph.go.th/data/AMR%202000-2022-12M.pdf
Parente DM, Morton J. Role of the pharmacist in antimicrobial stewardship. Med Clin North Am. 2018;102(5):929-36. doi: 10.1016/j.mcna.2018.05.009.
Tamma PD, Cosgrove SE. Antimicrobial stewardship. Infect Dis Clin North Am. 2011;25(1):245-60. doi: 10.1016/j.idc.2010.11.011.
Mathieu C, Pastene B, Cassir N, Martin-Loeches I, Leone M. Efficacy and safety of antimicrobial de-escalation as a clinical strategy. Expert Rev Anti Infect Ther. 2019;17(2):79-88. doi: 10.1080/14787210.2019.1561275.
Uda A, Tokimatsu I, Koike C, Osawa K, Shigemura K, Kimura T, et al. Antibiotic de-escalation therapy in patients with community-acquired nonbacteremic pneumococcal pneumonia. Int J Clin Pharm. 2019;41(6):1611-7. doi: 10.1007/s11096-019-00926-z.
Chotiprasitsakul D, Srichatrapimuk S, Kirdlarp S, Pyden AD, Santanirand P. Epidemiology of carbapenem-resistant Enterobacteriaceae: a 5-year experience at a tertiary care hospital. Infect Drug Resist. 2019;12:461-8. doi: 10.2147/IDR.S192540.
Gharbi M, Moore LS, Gilchrist M, Thomas CP, Bamford K, Brannigan ET, et al. Forecasting carbapenem resistance from antimicrobial consumption surveillance: lessons learnt from an OXA-48-producing Klebsiella pneumoniae outbreak in a West London renal unit. Int J Antimicrob Agents. 2015;46(2):150-6. doi: 10.1016/j.ijantimicag.2015.03.005.
สุภาพร คชายั่งยืน, พรวลัย บุญเมือง, วิชัย สันติมาลีวรกุล, วีรยุทธ์ แซ่ลิ้ม. การศึกษาผลลัพธ์ทางคลินิกและอัตราการตายในผู้ป่วยวิกฤตที่ได้รับยา meropenem จากภาวะพิษเหตุติดเชื้อ หรือภาวะช็อกจากพิษเหตุติดเชื้อ. ไทยไภษัชยนิพนธ์ [อินเทอร์เน็ต]. 2023 [สืบค้นเมื่อ 2 มี.ค. 2566];18(1):71-86. สืบค้นจาก: https://li01.tci-thaijo.org/index.php/TBPS/article/view/255812
Tamma PD, Aitken SL, Bonomo RA, Mathers AJ, Van Duin D, Clancy CJ. Infectious Diseases Society of America 2022 guidance on the treatment of extended-spectrum β-lactamase producing Enterobacterales (ESBL-E), carbapenem-resistant Enterobacterales (CRE), and Pseudomonas aeruginosa with difficult-to-treat resistance (DTR-P. aeruginosa). Clin Infect Dis. 2022;75(2):187-212. doi: 10.1093/cid/ciac268.
Gilbert DN, Chambers HF, Eliopoulos GM, Saag MS, Pavia AT, Black D. The Sanford guide to antimicrobial therapy 2022. 46th ed. n.p.: Antimicrobial Therapy, Inc; 2022.
Okada N, Azuma M, Tsujinaka K, Abe A, Takahashi M, Yano Y, et al. Clinical impact of a pharmacist-driven prospective audit with intervention and feedback on the treatment of patients with bloodstream infection. Antibiotics (Basel). 2022;11(9):1144. doi: 10.3390/antibiotics11091144.
Hammond KM, Kabbani D, Doucette KE, Smith SW, Lau C, Bains S, et al. How does the antimicrobial stewardship provider role affect prospective audit and feedback acceptance for restricted antibiotics in a Canadian tertiary-care center? Infection Control Hosp Epidemiol. 2024;45(2):234-6. doi: 10.1017/ice.2023.152.
Ohashi K, Matsuoka T, Shinoda Y, Mori T, Yoshida S, Yoshimura T, et al. Clinical outcome of pharmacist-led prospective audit with intervention and feedback after expansion from patients using specific antibiotics to those using whole injectable antibiotics. Eur J Clin Microbiol Infect Dis. 2019;38(3):593-600. doi: 10.1007/s10096-018-03465-z.
Lee RA, Stripling JT, Spellberg B, Centor RM. Short-course antibiotics for common infections: what do we know and where do we go from here? Clin Microbiol Infect. 2023;29(2):150-9. doi: 10.1016/j.cmi.2022.08.024.
Zhao X, Wu JF, Xiu QY, Wang C, Zhang DP, Huang JA, et al. A randomized controlled clinical trial of levofloxacin 750 mg versus 500 mg intravenous infusion in the treatment of community-acquired pneumonia. Diagn Microbiol Infect Dis. 2014;80(2):141-7. doi: 10.1016/j.diagmicrobio.2013.11.008.
van Nieuwkoop C, van der Starre WE, Stalenhoef JE, van Aartrijk AM, van der Reijden TJ, Vollaard AM, et al. Treatment duration of febrile urinary tract infection: a pragmatic randomized, double-blind, placebo-controlled non-inferiority trial in men and women. BMC Med. 2017;15(1):70. doi: 10.1186/s12916-017-0835-3.
Morley D, Torres A, Cillóniz C, Martin-Loeches I. Predictors of treatment failure and clinical stability in patients with community acquired pneumonia. Ann Transl Med. 2017;5(22):443. doi: 10.21037/atm.2017.06.54.
Carreno JJ, Kenney RM, Bloome M, McDonnell J, Rodriguez J, Weinmann A, et al. Evaluation of pharmacy generalists performing antimicrobial stewardship services. Am J Health Syst Pharm. 2015;72(15):1298-303. doi: 10.2146/ajhp140619.
Harris PNA, Tambyah PA, Lye DC, Mo Y, Lee TH, Yilmaz M, et al. Effect of piperacillin-tazobactam vs meropenem on 30-day mortality for patients with E coli or Klebsiella pneumoniae bloodstream infection and ceftriaxone resistance: a randomized clinical trial. JAMA. 2018;320(10):984-94. doi: 10.1001/jama.2018.12163.
ดาวน์โหลด
เผยแพร่แล้ว
วิธีการอ้างอิง
ฉบับ
บท
การอนุญาต
ลิขสิทธิ์ (c) 2025 กองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
วารสารเภสัชกรรมคลินิกเป็นวารสารในรูปแบบเปิด ผู้ใช้ทั่วไปสามารถเข้าถึง ดาวน์โหลด เอกสารไฟล์บทความบนเว็บไซต์วารสาร โดยไม่มีค่าใช้จ่ายแต่อย่างใด
ข้อความภายในบทความที่ตีพิมพ์ในวารสารเภสัชกรรมคลินิกทั้งหมด รวมถึงรูปภาพประกอบ ตาราง เป็นลิขสิทธิ์ของกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข อนุญาตให้นำไปใช้ประโยชน์และเผยแพร่ต่อได้โดยอยู่ภายใต้เงื่อนไขสัญญาอนุญาตครีเอทีฟคอมมอนส์ โดยต้องแสดงที่มาจากวารสาร – ไม่ใช้เพื่อการค้า – ห้ามแก้ไขดัดแปลง (Creative Commons Attribution-NonCommercial-NoDerivatives 4.0; CC BY-NC-ND 4.0) การนำเนื้อหา ข้อความหรือข้อคิดเห็น รูปภาพ ตาราง ของบทความไปจัดพิมพ์เผยแพร่ในรูปแบบต่าง ๆ เพื่อใช้ประโยชน์ในเชิงพาณิชย์ ต้องได้รับอนุญาตจากกองบรรณาธิการวารสารเภสัชกรรมคลินิกอย่างเป็นลายลักษณ์อักษร
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และบุคลากรในกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้เขียน ไม่เกี่ยวข้องกับกองบรรณาธิการ
