
สตีเวนส์จอห์นสันซินโดรมจากอัลโลพูรินอล ในผู้ป่วยชาวไทย ที่ผลเอชแอลเอ-บี*58:01 เป็นลบ: รายงานผู้ป่วย
คำสำคัญ:
สตีเวนส์จอห์นสันซินโดรม, อัลโลพูรินอล, เอชแอลเอ-บี*58:01บทคัดย่อ
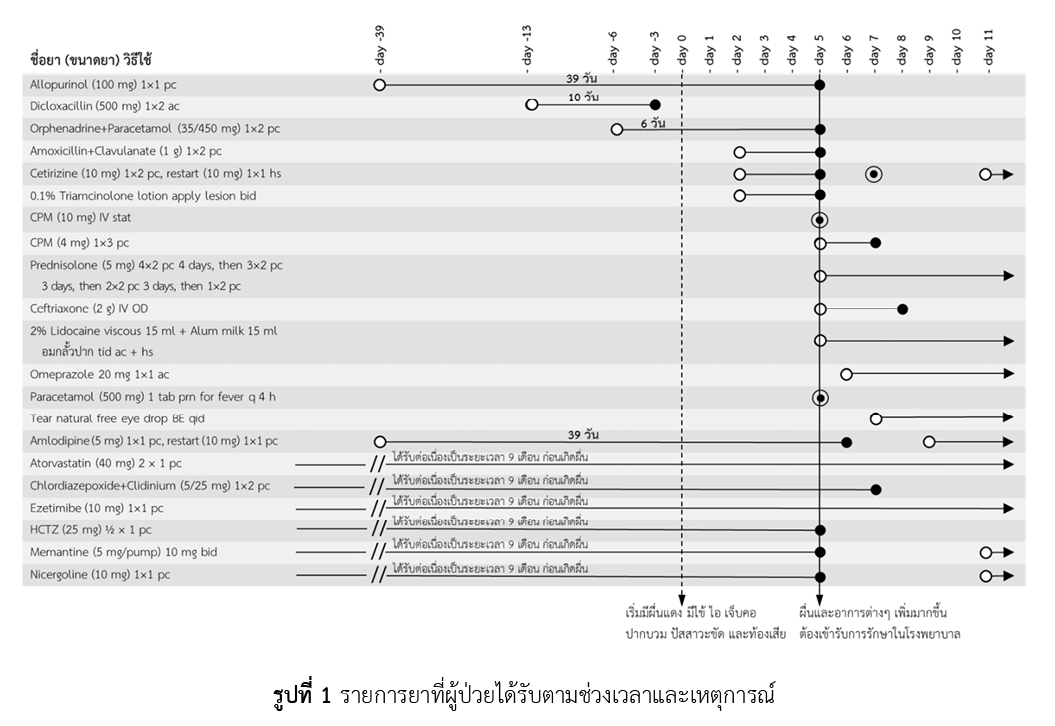
อัลโลพูรินอล เป็นยาลดกรดยูริกที่มีการใช้อย่างแพร่หลายสำหรับรักษาโรคเกาต์และภาวะกรดยูริกในเลือดสูง ทั้งยังเป็นสาเหตุสำคัญของการเกิดอาการไม่พึงประสงค์ทางผิวหนังชนิดรุนแรงจากยาในประเทศไทย โดยเฉพาะอาการแพ้ยาแบบสตีเวนส์จอห์นสันซินโดรม ซึ่งอาจนำมาสู่ความพิการหรือเสียชีวิตได้ ปัจจุบันมีการศึกษาค้นพบแล้วว่าการมียีน HLA-B*58:01 (ผลเป็นบวก) เป็นความเสี่ยงหนึ่งของการแพ้อัลโลพูรินอลแบบสตีเวนส์จอห์นสันซินโดรมทั้งในชาวเอเชียและยุโรป จึงได้มีคำแนะนำให้ตรวจคัดกรองยีน HLA-B*58:01 ก่อนเริ่มให้อัลโลพูรินอล เพื่อลดความเสี่ยงของการเกิดผื่นแพ้ยาชนิดรุนแรง แต่อย่างไรก็ตามรายงานผู้ป่วยฉบับนี้เป็นตัวอย่างผู้ป่วยหญิงไทยสูงอายุ ซึ่งได้รับการตรวจคัดกรองยีน HLA-B*58:01 ผลเป็นลบก่อนเริ่มอัลโลพูรินอลเนื่องจากภาวะกรดยูริกในเลือดสูงโดยที่ไม่มีอาการ แต่ผู้ป่วยเกิดอาการแพ้ยาแบบสตีเวนส์จอห์นสันซินโดรมหลังจากได้รับอัลโลพูรินอลเป็นเวลา 39 วัน ประเมินความสัมพันธ์ระหว่างการเกิดอาการไม่พึงประสงค์กับยาโดยใช้แบบประเมิน Naranjo's algorithm และ ALDEN ได้ผลการประเมินระดับน่าจะใช่ (probable ADR) จากอัลโลพูรินอล ผู้ป่วยต้องเข้ารับรักษาในโรงพยาบาลทั้งสิ้น 6 วัน ดังนั้นเพื่อความปลอดภัย แม้ว่าผลการตรวจคัดกรองยีน HLA-B*58:01 จะเป็นลบ ก็ควรต้องให้คำแนะนำ สังเกต และติดตามอาการผู้ป่วยอย่างใกล้ชิด โดยเฉพาะช่วง 1-3 เดือนแรกของการให้อัลโลพูรินอล
เอกสารอ้างอิง
Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998;279(15):1200-5. doi: 10.1001/jama.279.15.1200.
ศูนย์เฝ้าระวังความปลอดภัยด้านผลิตภัณฑ์สุขภาพ. ข่าวสารประชาสัมพันธ์ศูนย์เฝ้าระวังความปลอดภัยด้านผลิตภัณฑ์สุขภาพ: สรุปรายงานอาการไม่พึงประสงค์จากการใช้ยา ประจำปี 2564 [อินเทอร์เน็ต]. กรุงเทพมหานคร: ศูนย์เฝ้าระวังความปลอดภัยด้านผลิตภัณฑ์สุขภาพ กองยุทธศาสตร์และแผนงาน สำนักงานคณะกรรมการอาหารและยา; 2565 [สืบค้นเมื่อ 13 ก.ค. 2566]. สืบค้นจาก: https://hpvc.fda.moph.go.th/AEINFO/NewsPublishView.aspx?ID=12620
Svensson CK, Cowen EW, Gaspari AA. Cutaneous drug reactions. Pharmacol Rev. 2001;53(3):357-79. PMID: 11546834.
Harr T, French LE. Toxic epidermal necrolysis and Stevens-Johnson syndrome. Orphanet J Rare Dis. 2010;5:39. doi: 10.1186/1750-1172-5-39.
Roujeau JC, Kelly JP, Naldi L, Rzany B, Stern RS, Anderson T, et al. Medication use and the risk of Stevens–Johnson syndrome or toxic epidermal necrolysis. N Engl J Med. 1995;333(24):1600-7. doi: 10.1056/NEJM199512143332404.
Pan RY, Dao RL, Hung SI, Chung WH. Pharmacogenomic advances in the prediction and prevention of cutaneous idiosyncratic drug reactions. Clin Pharmacol Ther. 2017;102(1):86-97. doi: 10.1002/cpt.683.
Limkobpaiboon S, Panomvanna Na Ayudhya D, Dhana N, Jongjarearnprasert K. Prevalence and mortality rate of severe cutaneous adverse reactions at Siriraj Hospital. Chula Med J. 2010;54(5):467-77. doi: 10.58837/CHULA.CMJ.54.5.7.
Dilokthornsakul P, Sawangjit R, Inprasong C, Chunhasewee S, Rattanapan P, Thoopputra T, et al. Healthcare utilization and cost of Stevens-Johnson syndrome and toxic epidermal necrolysis management in Thailand. J Postgrad Med. 2016;62(2):109-14. doi: 10.4103/0022-3859.
Day RO, Graham GG, Hicks M, McLachlan AJ, Stocker SL, Williams KM. Clinical pharmacokinetics and pharmacodynamics of allopurinol and oxypurinol. Clin Pharmacokinet. 2007;46(8):623-44. doi: 10.2165/00003088-200746080-00001.
FitzGerald JD, Dalbeth N, Mikuls T, Brignardello-Petersen R, Guyatt G, Abeles AM, et al. 2020 American College of Rheumatology guideline for the management of gout. Arthritis Care Res (Hoboken). 2020;72(6):744-60. doi: 10.1002/acr.24180.
Roujeau JC, Stern RS. Severe adverse cutaneous reactions to drugs. N Engl J Med. 1994;331(19):1272-85. doi: 10.1056/NEJM199411103311906.
Hung SI, Chung WH, Liou LB, Chu CC, Lin M, Huang HP, et al. HLA-B*5801 allele as a genetic marker for severe cutaneous adverse reactions caused by allopurinol. Proc Natl Acad Sci U S A. 2005;102(11):4134-9. doi: 10.1073/pnas.0409500102.
Cao ZH, Wei ZY, Zhu QY, Zhang JY, Yang L, Qin SY, et al. HLA-B*58:01 allele is associated with augmented risk for both mild and severe cutaneous adverse reactions induced by allopurinol in Han Chinese. Pharmacogenomics. 2012;13(10):1193-201. doi: 10.2217/pgs.12.89.
Tassaneeyakul W, Jantararoungtong T, Chen P, Lin PY, Tiamkao S, Khunarkornsiri U, et al. Strong association between HLA-B*5801 and allopurinol-induced Stevens-Johnson syndrome and toxic epidermal necrolysis in a Thai population. Pharmacogenet Genomics. 2009;19(9):704-9. doi: 10.1097/FPC.0b013e328330a3b8.
Limkobpaiboon S, Panomvana D, Koolvisut A, Vejbaesya S. Association between HLA-B*5801 allele and other risk factors to allopurinol - induced severe cutaneous adverse reaction and exfoliative dermatitis in Thai population. Int J Pharm [Internet]. 2013 [cited 2023 Jun 13];3(4):692-7. Available from: https://citeseerx.ist.psu.edu/document?repid=rep1&type=pdf&doi=0d98c8171a469b5d269b0090db8799742802f934
Sukasem C, Jantararoungtong T, Kuntawong P, Puangpetch A, Koomdee N, Satapornpong P, et al. HLA-B (*) 58:01 for allopurinol-induced cutaneous adverse drug reactions: implication for clinical interpretation in Thailand. Front Pharmacol. 2016;7:186. doi: 10.3389/fphar.2016.00186.
Kaniwa N, Saito Y, Aihara M, Matsunaga K, Tohkin M, Kurose K, et al. HLA-B locus in Japanese patients with anti-epileptics and allopurinol-related Stevens-Johnson syndrome and toxic epidermal necrolysis. Pharmacogenomics. 2008;9(11):1617-22. doi: 10.2217/14622416.9.11.1617.
Niihara H, Kaneko S, Ito T, Sugamori T, Takahashi N, Kohno K, et al. HLA-B*58:01 strongly associates with allopurinol-induced adverse drug reactions in a Japanese sample population. J Dermatol Sci. 2013;71(2):150-2. doi: 10.1016/j.jdermsci.2013.04.013.
Kang HR, Jee YK, Kim YS, Lee CH, Jung JW, Kim SH, et al. Positive and negative associations of HLA class I alleles with allopurinol-induced SCARs in Koreans. Pharmacogenet Genomics. 2011;21(5):303-7. doi: 10.1097/FPC.0b013e32834282b8.
Lonjou C, Borot N, Sekula P, Ledger N, Thomas L, Halevy S, et al. A European study of HLA-B in Stevens-Johnson syndrome and toxic epidermal necrolysis related to five high-risk drugs. Pharmacogenet Genomics. 2008;18(2):99-107. doi: 10.1097/FPC.0b013e3282f3ef9c.
Gonçalo M, Coutinho I, Teixeira V, Gameiro AR, Brites MM, Nunes R, et al. HLA-B*58:01 is a risk factor for allopurinol-induced DRESS and Stevens-Johnson syndrome/toxic epidermal necrolysis in a Portuguese population. Br J Dermatol. 2013;169(3):660-5. doi: 10.1111/bjd.12389.
Hershfield MS, Callaghan JT, Tassaneeyakul W, Mushiroda T, Thorn CF, Klein TE, et al. Clinical Pharmacogenetics Implementation Consortium guidelines for human leukocyte antigen-B genotype and allopurinol dosing. Clin Pharmacol Ther. 2013;93(2):153-8. doi: 10.1038/clpt.2012.209.
Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239-45. doi: 10.1038/clpt.1981.154.
Sassolas B, Haddad C, Mockenhaupt M, Dunant A, Liss Y, Bork K, et al. ALDEN, an algorithm for assessment of drug causality in Stevens-Johnson syndrome and toxic epidermal necrolysis: comparison with case-control analysis. Clin Pharmacol Ther. 2010;88(1):60-8. doi: 10.1038/clpt.2009.252.
Mockenhaupt M, Viboud C, Dunant A, Naldi L, Halevy S, Bouwes Bavinck JN, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: assessment of medication risks with emphasis on recently marketed drugs. The EuroSCAR-study. J Invest Dermatol. 2008;128(1):35-44. doi: 10.1038/sj.jid.5701033.
Sukasem C, Tempark T. Pharmacogenomics: a new approach for preventing severe cutaneous adverse drug reactions. In: Pathak Y, editor. Genomics-driven healthcare: trends in disease prevention and treatment. Singapore: Adis, Singapore; 2018. p. 373-409. doi: 10.1007/978-981-10-7506-3_18
Yun J, Marcaida MJ, Eriksson KK, Jamin H, Fontana S, Pichler WJ, et al. Oxypurinol directly and immediately activates the drug-specific T cells via the preferential use of HLA-B*58:01. J Immunol. 2014;192(7):2984-93. doi: 10.4049/jimmunol.1302306.
Kim MY, Yun J, Kang DY, Kim TH, Oh MK, Lee S, et al. HLA-A*24:02 increase the risk of allopurinol-induced drug reaction with eosinophilia and systemic symptoms in HLA-B*58:01 carriers in a Korean population; a multicenter cross-sectional case-control study. Clin Transl Allergy. 2022;12(9):e12193. doi: 10.1002/clt2.12193.
Saksit N, Tassaneeyakul W, Nakkam N, Konyoung P, Khunarkornsiri U, Chumworathayi P, et al. Risk factors of allopurinol-induced severe cutaneous adverse reactions in a Thai population. Pharmacogenet Genomics. 2017;27(7):255-63. doi: 10.1097/FPC.0000000000000285.
Saokaew S, Tassaneeyakul W, Maenthaisong R, Chaiyakunapruk N. Cost-effectiveness analysis of HLA-B*5801 testing in preventing allopurinol-induced SJS/TEN in Thai population. PLoS One. 2014;9(4):e94294. doi: 10.1371/journal.pone.0094294.
ดาวน์โหลด
เผยแพร่แล้ว
วิธีการอ้างอิง
ฉบับ
บท
การอนุญาต
ลิขสิทธิ์ (c) 2024 กองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
วารสารเภสัชกรรมคลินิกเป็นวารสารในรูปแบบเปิด ผู้ใช้ทั่วไปสามารถเข้าถึง ดาวน์โหลด เอกสารไฟล์บทความบนเว็บไซต์วารสาร โดยไม่มีค่าใช้จ่ายแต่อย่างใด
ข้อความภายในบทความที่ตีพิมพ์ในวารสารเภสัชกรรมคลินิกทั้งหมด รวมถึงรูปภาพประกอบ ตาราง เป็นลิขสิทธิ์ของกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข อนุญาตให้นำไปใช้ประโยชน์และเผยแพร่ต่อได้โดยอยู่ภายใต้เงื่อนไขสัญญาอนุญาตครีเอทีฟคอมมอนส์ โดยต้องแสดงที่มาจากวารสาร – ไม่ใช้เพื่อการค้า – ห้ามแก้ไขดัดแปลง (Creative Commons Attribution-NonCommercial-NoDerivatives 4.0; CC BY-NC-ND 4.0) การนำเนื้อหา ข้อความหรือข้อคิดเห็น รูปภาพ ตาราง ของบทความไปจัดพิมพ์เผยแพร่ในรูปแบบต่าง ๆ เพื่อใช้ประโยชน์ในเชิงพาณิชย์ ต้องได้รับอนุญาตจากกองบรรณาธิการวารสารเภสัชกรรมคลินิกอย่างเป็นลายลักษณ์อักษร
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และบุคลากรในกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้เขียน ไม่เกี่ยวข้องกับกองบรรณาธิการ
