Allopurinol-Induced Stevens-Johnson Syndrome in a Thai Patient with HLA-B*58:01 Negative: A Case Report
Keywords:
Stevens-Johnson syndrome, HLA-B*58:01, allopurinolAbstract
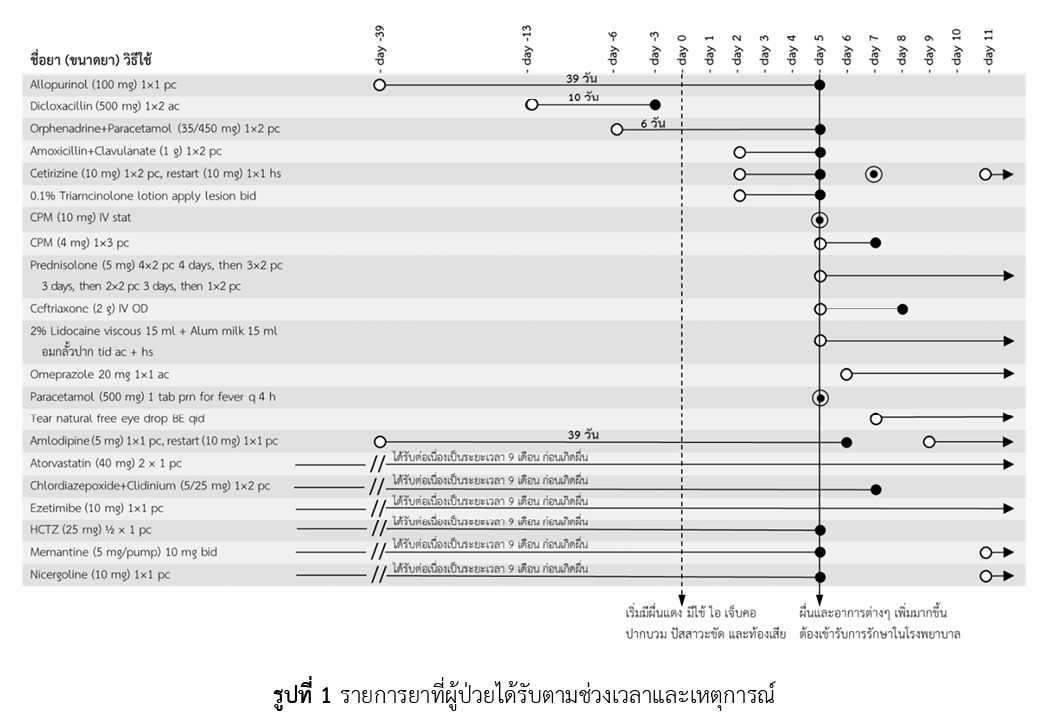
Allopurinol is a uric-lowering agent widely used to treat gout and hyperuricemia. However, allopurinol is also the leading cause of severe cutaneous adverse drug reactions in Thailand, particularly Stevens-Johnson syndrome, which may lead to disability or death. Current studies have found that the presence of the HLA-B*58:01 gene (positive result) is a risk factor for allopurinol-induced Stevens-Johnson syndrome in Asian and European populations. Consequently, screening for the HLA-B*58:01 gene before initiating allopurinol is recommended to reduce the risk of severe cutaneous drug eruptions. This report presents a case of an elderly Thai female patient who developed Stevens-Johnson syndrome after 39 days of allopurinol administration to treat asymptomatic hyperuricemia. However, her HLA-B*58:01 gene screening before starting allopurinol was negative. The result of the causality assessment of adverse drug reactions using Naranjo's algorithm and ALDEN was a probable ADR due to allopurinol. She had to stay hospitalized for a total of 6 days for treatment. Therefore, for safety, even if the HLA-B*58:01 gene screening result is negative, patient advice, observation, and close drug monitoring should be provided, especially during the first 1-3 months of allopurinol administration.
References
Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA. 1998;279(15):1200-5. doi: 10.1001/jama.279.15.1200.
ศูนย์เฝ้าระวังความปลอดภัยด้านผลิตภัณฑ์สุขภาพ. ข่าวสารประชาสัมพันธ์ศูนย์เฝ้าระวังความปลอดภัยด้านผลิตภัณฑ์สุขภาพ: สรุปรายงานอาการไม่พึงประสงค์จากการใช้ยา ประจำปี 2564 [อินเทอร์เน็ต]. กรุงเทพมหานคร: ศูนย์เฝ้าระวังความปลอดภัยด้านผลิตภัณฑ์สุขภาพ กองยุทธศาสตร์และแผนงาน สำนักงานคณะกรรมการอาหารและยา; 2565 [สืบค้นเมื่อ 13 ก.ค. 2566]. สืบค้นจาก: https://hpvc.fda.moph.go.th/AEINFO/NewsPublishView.aspx?ID=12620
Svensson CK, Cowen EW, Gaspari AA. Cutaneous drug reactions. Pharmacol Rev. 2001;53(3):357-79. PMID: 11546834.
Harr T, French LE. Toxic epidermal necrolysis and Stevens-Johnson syndrome. Orphanet J Rare Dis. 2010;5:39. doi: 10.1186/1750-1172-5-39.
Roujeau JC, Kelly JP, Naldi L, Rzany B, Stern RS, Anderson T, et al. Medication use and the risk of Stevens–Johnson syndrome or toxic epidermal necrolysis. N Engl J Med. 1995;333(24):1600-7. doi: 10.1056/NEJM199512143332404.
Pan RY, Dao RL, Hung SI, Chung WH. Pharmacogenomic advances in the prediction and prevention of cutaneous idiosyncratic drug reactions. Clin Pharmacol Ther. 2017;102(1):86-97. doi: 10.1002/cpt.683.
Limkobpaiboon S, Panomvanna Na Ayudhya D, Dhana N, Jongjarearnprasert K. Prevalence and mortality rate of severe cutaneous adverse reactions at Siriraj Hospital. Chula Med J. 2010;54(5):467-77. doi: 10.58837/CHULA.CMJ.54.5.7.
Dilokthornsakul P, Sawangjit R, Inprasong C, Chunhasewee S, Rattanapan P, Thoopputra T, et al. Healthcare utilization and cost of Stevens-Johnson syndrome and toxic epidermal necrolysis management in Thailand. J Postgrad Med. 2016;62(2):109-14. doi: 10.4103/0022-3859.
Day RO, Graham GG, Hicks M, McLachlan AJ, Stocker SL, Williams KM. Clinical pharmacokinetics and pharmacodynamics of allopurinol and oxypurinol. Clin Pharmacokinet. 2007;46(8):623-44. doi: 10.2165/00003088-200746080-00001.
FitzGerald JD, Dalbeth N, Mikuls T, Brignardello-Petersen R, Guyatt G, Abeles AM, et al. 2020 American College of Rheumatology guideline for the management of gout. Arthritis Care Res (Hoboken). 2020;72(6):744-60. doi: 10.1002/acr.24180.
Roujeau JC, Stern RS. Severe adverse cutaneous reactions to drugs. N Engl J Med. 1994;331(19):1272-85. doi: 10.1056/NEJM199411103311906.
Hung SI, Chung WH, Liou LB, Chu CC, Lin M, Huang HP, et al. HLA-B*5801 allele as a genetic marker for severe cutaneous adverse reactions caused by allopurinol. Proc Natl Acad Sci U S A. 2005;102(11):4134-9. doi: 10.1073/pnas.0409500102.
Cao ZH, Wei ZY, Zhu QY, Zhang JY, Yang L, Qin SY, et al. HLA-B*58:01 allele is associated with augmented risk for both mild and severe cutaneous adverse reactions induced by allopurinol in Han Chinese. Pharmacogenomics. 2012;13(10):1193-201. doi: 10.2217/pgs.12.89.
Tassaneeyakul W, Jantararoungtong T, Chen P, Lin PY, Tiamkao S, Khunarkornsiri U, et al. Strong association between HLA-B*5801 and allopurinol-induced Stevens-Johnson syndrome and toxic epidermal necrolysis in a Thai population. Pharmacogenet Genomics. 2009;19(9):704-9. doi: 10.1097/FPC.0b013e328330a3b8.
Limkobpaiboon S, Panomvana D, Koolvisut A, Vejbaesya S. Association between HLA-B*5801 allele and other risk factors to allopurinol - induced severe cutaneous adverse reaction and exfoliative dermatitis in Thai population. Int J Pharm [Internet]. 2013 [cited 2023 Jun 13];3(4):692-7. Available from: https://citeseerx.ist.psu.edu/document?repid=rep1&type=pdf&doi=0d98c8171a469b5d269b0090db8799742802f934
Sukasem C, Jantararoungtong T, Kuntawong P, Puangpetch A, Koomdee N, Satapornpong P, et al. HLA-B (*) 58:01 for allopurinol-induced cutaneous adverse drug reactions: implication for clinical interpretation in Thailand. Front Pharmacol. 2016;7:186. doi: 10.3389/fphar.2016.00186.
Kaniwa N, Saito Y, Aihara M, Matsunaga K, Tohkin M, Kurose K, et al. HLA-B locus in Japanese patients with anti-epileptics and allopurinol-related Stevens-Johnson syndrome and toxic epidermal necrolysis. Pharmacogenomics. 2008;9(11):1617-22. doi: 10.2217/14622416.9.11.1617.
Niihara H, Kaneko S, Ito T, Sugamori T, Takahashi N, Kohno K, et al. HLA-B*58:01 strongly associates with allopurinol-induced adverse drug reactions in a Japanese sample population. J Dermatol Sci. 2013;71(2):150-2. doi: 10.1016/j.jdermsci.2013.04.013.
Kang HR, Jee YK, Kim YS, Lee CH, Jung JW, Kim SH, et al. Positive and negative associations of HLA class I alleles with allopurinol-induced SCARs in Koreans. Pharmacogenet Genomics. 2011;21(5):303-7. doi: 10.1097/FPC.0b013e32834282b8.
Lonjou C, Borot N, Sekula P, Ledger N, Thomas L, Halevy S, et al. A European study of HLA-B in Stevens-Johnson syndrome and toxic epidermal necrolysis related to five high-risk drugs. Pharmacogenet Genomics. 2008;18(2):99-107. doi: 10.1097/FPC.0b013e3282f3ef9c.
Gonçalo M, Coutinho I, Teixeira V, Gameiro AR, Brites MM, Nunes R, et al. HLA-B*58:01 is a risk factor for allopurinol-induced DRESS and Stevens-Johnson syndrome/toxic epidermal necrolysis in a Portuguese population. Br J Dermatol. 2013;169(3):660-5. doi: 10.1111/bjd.12389.
Hershfield MS, Callaghan JT, Tassaneeyakul W, Mushiroda T, Thorn CF, Klein TE, et al. Clinical Pharmacogenetics Implementation Consortium guidelines for human leukocyte antigen-B genotype and allopurinol dosing. Clin Pharmacol Ther. 2013;93(2):153-8. doi: 10.1038/clpt.2012.209.
Naranjo CA, Busto U, Sellers EM, Sandor P, Ruiz I, Roberts EA, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239-45. doi: 10.1038/clpt.1981.154.
Sassolas B, Haddad C, Mockenhaupt M, Dunant A, Liss Y, Bork K, et al. ALDEN, an algorithm for assessment of drug causality in Stevens-Johnson syndrome and toxic epidermal necrolysis: comparison with case-control analysis. Clin Pharmacol Ther. 2010;88(1):60-8. doi: 10.1038/clpt.2009.252.
Mockenhaupt M, Viboud C, Dunant A, Naldi L, Halevy S, Bouwes Bavinck JN, et al. Stevens-Johnson syndrome and toxic epidermal necrolysis: assessment of medication risks with emphasis on recently marketed drugs. The EuroSCAR-study. J Invest Dermatol. 2008;128(1):35-44. doi: 10.1038/sj.jid.5701033.
Sukasem C, Tempark T. Pharmacogenomics: a new approach for preventing severe cutaneous adverse drug reactions. In: Pathak Y, editor. Genomics-driven healthcare: trends in disease prevention and treatment. Singapore: Adis, Singapore; 2018. p. 373-409. doi: 10.1007/978-981-10-7506-3_18
Yun J, Marcaida MJ, Eriksson KK, Jamin H, Fontana S, Pichler WJ, et al. Oxypurinol directly and immediately activates the drug-specific T cells via the preferential use of HLA-B*58:01. J Immunol. 2014;192(7):2984-93. doi: 10.4049/jimmunol.1302306.
Kim MY, Yun J, Kang DY, Kim TH, Oh MK, Lee S, et al. HLA-A*24:02 increase the risk of allopurinol-induced drug reaction with eosinophilia and systemic symptoms in HLA-B*58:01 carriers in a Korean population; a multicenter cross-sectional case-control study. Clin Transl Allergy. 2022;12(9):e12193. doi: 10.1002/clt2.12193.
Saksit N, Tassaneeyakul W, Nakkam N, Konyoung P, Khunarkornsiri U, Chumworathayi P, et al. Risk factors of allopurinol-induced severe cutaneous adverse reactions in a Thai population. Pharmacogenet Genomics. 2017;27(7):255-63. doi: 10.1097/FPC.0000000000000285.
Saokaew S, Tassaneeyakul W, Maenthaisong R, Chaiyakunapruk N. Cost-effectiveness analysis of HLA-B*5801 testing in preventing allopurinol-induced SJS/TEN in Thai population. PLoS One. 2014;9(4):e94294. doi: 10.1371/journal.pone.0094294.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2024 Health Administration Division, Office of the Permanent Secretary, Ministry of Public Health and The Society of Hospital Pharmacist, Ministry of Public Health

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
วารสารเภสัชกรรมคลินิกเป็นวารสารในรูปแบบเปิด ผู้ใช้ทั่วไปสามารถเข้าถึง ดาวน์โหลด เอกสารไฟล์บทความบนเว็บไซต์วารสาร โดยไม่มีค่าใช้จ่ายแต่อย่างใด
ข้อความภายในบทความที่ตีพิมพ์ในวารสารเภสัชกรรมคลินิกทั้งหมด รวมถึงรูปภาพประกอบ ตาราง เป็นลิขสิทธิ์ของกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข อนุญาตให้นำไปใช้ประโยชน์และเผยแพร่ต่อได้โดยอยู่ภายใต้เงื่อนไขสัญญาอนุญาตครีเอทีฟคอมมอนส์ โดยต้องแสดงที่มาจากวารสาร – ไม่ใช้เพื่อการค้า – ห้ามแก้ไขดัดแปลง (Creative Commons Attribution-NonCommercial-NoDerivatives 4.0; CC BY-NC-ND 4.0) การนำเนื้อหา ข้อความหรือข้อคิดเห็น รูปภาพ ตาราง ของบทความไปจัดพิมพ์เผยแพร่ในรูปแบบต่าง ๆ เพื่อใช้ประโยชน์ในเชิงพาณิชย์ ต้องได้รับอนุญาตจากกองบรรณาธิการวารสารเภสัชกรรมคลินิกอย่างเป็นลายลักษณ์อักษร
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และบุคลากรในกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้เขียน ไม่เกี่ยวข้องกับกองบรรณาธิการ
