
ผลกระทบของภาวะเลือดออกรุนแรงจากการใช้ยาวาร์ฟารินในผู้ป่วยหัวใจเต้นผิดจังหวะต่อการเข้ารับการรักษาในโรงพยาบาลและต้นทุนทางตรงในผู้ป่วยสูงอายุในประเทศไทย
คำสำคัญ:
หัวใจเต้นผิดจังหวะ, วาร์ฟาริน, ภาวะเลือดออกรุนแรง, ผู้สูงอายุบทคัดย่อ
ความเป็นมา: วาร์ฟารินเป็นยาหลักในการป้องกันภาวะลิ่มเลือดอุดตันในผู้ป่วยหัวใจเต้นผิดจังหวะในประเทศไทย แต่มีความเสี่ยงต่อภาวะเลือดออกรุนแรง (major bleeding) โดยเฉพาะในผู้สูงอายุที่มีการเปลี่ยนแปลงทางเภสัชจลนศาสตร์ การทำงานของตับและไตที่ลดลง รวมทั้งมีโรคร่วมและการใช้ยาหลายชนิดที่ส่งผลให้ระดับยาสูงขึ้น ค่า INR เกินเป้าหมาย นำไปสู่การเข้ารักษาตัวและเพิ่มภาระค่าใช้จ่ายทางการแพทย์ ในโรงพยาบาลพุทธชินราช พิษณุโลก พบว่า 1 ใน 3 ของผู้ป่วยที่ได้รับวาร์ฟารินมีอายุ ≥75 ปี แต่ยังไม่มีข้อมูลอุบัติการณ์และผลกระทบ จึงเป็นเหตุผลสำคัญในการศึกษานี้
วัตถุประสงค์: เพื่อเปรียบเทียบภาวะเลือดออกรุนแรงในผู้ป่วยหัวใจเต้นผิดจังหวะระหว่างอายุ 65-74 ปี กับอายุ ≥75 ปี
วิธีวิจัย: ศึกษาแบบย้อนหลังในผู้ป่วยหัวใจเต้นผิดจังหวะที่ใช้วาร์ฟารินในโรงพยาบาลพุทธชินราช ระหว่าง 1 มกราคม พ.ศ. 2562 - 31 มกราคม พ.ศ. 2565 ศึกษาอุบัติการณ์ภาวะเลือดออกรุนแรง ระยะเวลานอนโรงพยาบาล และต้นทุนทางตรงจากฐานข้อมูลโรงพยาบาลและโปรแกรม Warfarin Registry Network
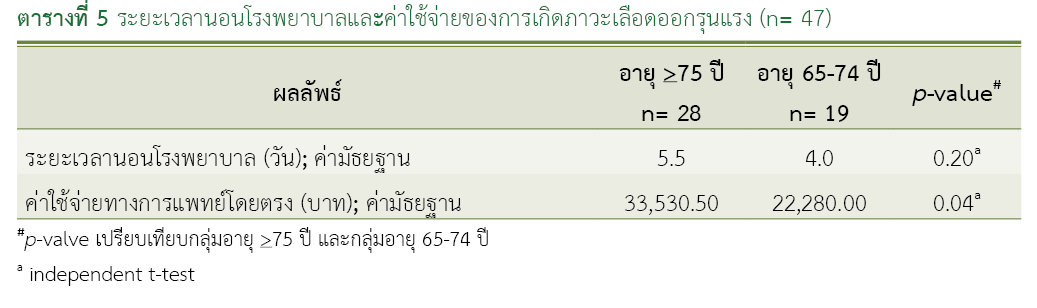
ผลการวิจัย: ผู้ป่วย 645 ราย อายุเฉลี่ย 75.75 ± 7.24 ปี คะแนน CHA2DS2-VASc เฉลี่ย 3.54 ± 1.10 อุบัติการณ์ภาวะเลือดออกรุนแรงในกลุ่มอายุ ≥75 ปี 8.35% (28 ราย) เทียบกับ 6.12% (19 ราย) ในกลุ่มอายุ 65-74 ปี ค่ามัธยฐานวันนอนโรงพยาบาล 5.5 วัน เทียบกับ 4 วัน (p-value = 0.20) ค่ามัธยฐานต้นทุนทางตรง 33,530.50 บาท เทียบกับ 22,280.00 บาท แตกต่างกันอย่างมีนัยสำคัญทางสถิติ (p-value = 0.04)
สรุปผลการวิจัย: ผู้ป่วยหัวใจเต้นผิดจังหวะที่ใช้วาร์ฟารินอายุ ≥75 ปี มีโอกาสเกิดอุบัติการณ์ภาวะเลือดออกรุนแรงสูงกว่ากลุ่ม 65-74 ปี ไม่แตกต่างกันอย่างมีนัยสำคัญทางสถิติ แต่เพิ่มต้นทุนทางตรงในการรักษาอย่างมีนัยสำคัญทางสถิติ
เอกสารอ้างอิง
Krittayaphong R, Boonyapiphat T, Wongvipaporn C, Sairat P. Age-related clinical outcomes of patients with non-valvular atrial fibrillation: insights from the COOL-AF. Clin Interv Aging. 2021;16:707-19. doi: 10.2147/CIA.S302389.
Phrommintikul A, Detnuntarat P, Prasertwitayakij N, Wongcharoen W. Prevalence of atrial fibrillation in Thai elderly. J Geriatr Cardiol. 2016;13(3):270-3. doi: 10.11909/j.issn.1671-5411.2016.03.002.
Ghate SR, Biskupiak J, Ye X, Kwong WJ, Brixner DI. All-cause and bleeding-related health care costs in warfarin-treated patients with atrial fibrillation. J Manag Care Pharm. 2011;17(9):672-84. doi: 10.18553/jmcp.2011.17.9.672.
Roberts KM, Knight TB, Padilla-Tolentino E, Murthy M, Peterson EJ. Length of stay comparison between rivaroxaban and warfarin in the treatment of pulmonary embolism: results from a real-World observational cohort study. Thrombosis. 2015;2015:414523. doi: 10.1155/2015/414523.
Charlton B, Adeboyeje G, Barron JJ, Grady D, Shin J, Redberg RF. Length of hospitalization and mortality for bleeding during treatment with warfarin, dabigatran, or rivaroxaban. PLoS One. 2018;13(3):e0193912. doi: 10.1371/journal.pone.0193912.
George D, Wong CA, Thanimalai S, Tan HS. Severity and hospitalization cost related to warfarin-related adverse events in a tertiary Malaysian hospital. Hosp Pharm. 2022;57(5):633–8. doi: 10.1177/00185787211070182.
Hylek EM, Evans-Molina C, Shea C, Henault LE, Regan S. Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation. 2007;115(21):2689-96. doi: 10.1161/CIRCULATIONAHA.106.653048.
Franco L, Becattini C, Beyer-Westendorf J, Vanni S, Nitti C, Re R, et al. Definition of major bleeding: prognostic classification. J Thromb Haemost. 2020;18(11):2852-60. doi: 10.1111/jth.15048.
Lan Y, Chen J, Niu P, Huang X, Dong X, You C, et al. Efficacy, safety, and bleeding risk factor analysis of oral anticoagulants in AF patients ≥ 65 years of age: a multicenter retrospective cohort study. BMC Geriatr. 2025;25(1):203. doi: 10.1186/s12877-025-05838-4.
Rydberg DM, Linder M, Malmström RE, Andersen M. Risk factors for severe bleeding events during warfarin treatment: the influence of sex, age, comorbidity, and co-medication. Eur J Clin Pharmacol. 2020;76(6):867-76. doi: 10.1007/s00228-020-02856-6.
Hicks KA, Stockbridge NL, Targum SL, Temple RJ. Bleeding Academic Research Consortium consensus report: the Food and Drug Administration perspective.Circulation. 2011;123(23):2664-5. doi: 10.1161/CIRCULATIONAHA.111.032433.
Palareti G, Hirsh J, Legnani C, Manotti C, D'Angelo A, Pengo V, et al. Oral anticoagulation treatment in the elderly: a nested, prospective, case-control study. Arch Intern Med. 2000;160(4):470-8. doi: 10.1001/archinte.160.4.470.
Priksri W, Rattanavipanon W, Saejear W, Tanyasaensook K, Phrommintikul A, Chulavatnatol S, et al. Incidence, risk factors, and outcomes of warfarin-associated major bleeding in Thai population. Pharmacoepidemiol Drug Saf. 2019;28(7):942-50. doi: 10.1002/pds.4781.
ดาวน์โหลด
เผยแพร่แล้ว
วิธีการอ้างอิง
ฉบับ
บท
การอนุญาต
ลิขสิทธิ์ (c) 2025 กองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
วารสารเภสัชกรรมคลินิกเป็นวารสารในรูปแบบเปิด ผู้ใช้ทั่วไปสามารถเข้าถึง ดาวน์โหลด เอกสารไฟล์บทความบนเว็บไซต์วารสาร โดยไม่มีค่าใช้จ่ายแต่อย่างใด
ข้อความภายในบทความที่ตีพิมพ์ในวารสารเภสัชกรรมคลินิกทั้งหมด รวมถึงรูปภาพประกอบ ตาราง เป็นลิขสิทธิ์ของกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข อนุญาตให้นำไปใช้ประโยชน์และเผยแพร่ต่อได้โดยอยู่ภายใต้เงื่อนไขสัญญาอนุญาตครีเอทีฟคอมมอนส์ โดยต้องแสดงที่มาจากวารสาร – ไม่ใช้เพื่อการค้า – ห้ามแก้ไขดัดแปลง (Creative Commons Attribution-NonCommercial-NoDerivatives 4.0; CC BY-NC-ND 4.0) การนำเนื้อหา ข้อความหรือข้อคิดเห็น รูปภาพ ตาราง ของบทความไปจัดพิมพ์เผยแพร่ในรูปแบบต่าง ๆ เพื่อใช้ประโยชน์ในเชิงพาณิชย์ ต้องได้รับอนุญาตจากกองบรรณาธิการวารสารเภสัชกรรมคลินิกอย่างเป็นลายลักษณ์อักษร
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และบุคลากรในกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้เขียน ไม่เกี่ยวข้องกับกองบรรณาธิการ
