Effects of Warfarin-Related Major Bleeding Adverse Events to Hospitalization and Direct Costs in Elderly Patients in Thailand
Keywords:
atrial fibrillation, warfarin, major bleeding, elderlyAbstract
Background: Warfarin remains the first-line therapy for thromboembolism prevention in Thai patients with atrial fibrillation but carries major bleeding risks, particularly among elderly patients who experience age-related pharmacokinetic changes, declining hepatic and renal function, and polypharmacy. These factors increase warfarin levels, leading to supratherapeutic INR, hospitalization, and higher healthcare costs. At Buddhachinaraj Phitsanulok Hospital, one-third of warfarin-treated patients are aged ≥75 years; however, no data currently exist regarding the incidence and outcomes of adverse events in this population.
Objective: To compare the risk of major bleeding between atrial fibrillation patients aged 65–74 years and those aged ≥75 years.
Methods: This retrospective cohort study included atrial fibrillation patients receiving warfarin at Buddhachinaraj Phitsanulok Hospital between January 1, 2019, and January 31, 2022. Data on major bleeding incidence, hospital length of stay, and direct medical costs were obtained from hospital databases and the Warfarin Registry Network.
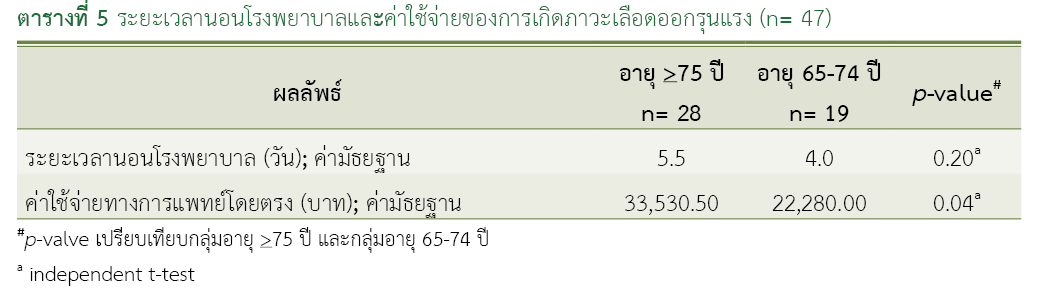
Results: Among 645 patients (mean age 75.75 ± 7.24 years; mean CHA2DS2-VASc score 3.54 ± 1.10), major bleeding occurred in 8.35% (28 patients) of the ≥75-year group and 6.12% (19 patients) of the 65–74-year group. The median length of stay was 5.5 versus 4.0 days (p-value = 0.20). Median direct medical costs were significantly higher in the ≥75-year group (THB 33,530.50) compared with the 65–74-year group (THB 22,280.00; p-value = 0.04).
Conclusions: Among warfarin-treated patients with atrial fibrillation, those aged ≥75 years had a higher, though not statistically significant, incidence of major bleeding and significantly greater direct medical costs than those aged 65–74 years.
References
Krittayaphong R, Boonyapiphat T, Wongvipaporn C, Sairat P. Age-related clinical outcomes of patients with non-valvular atrial fibrillation: insights from the COOL-AF. Clin Interv Aging. 2021;16:707-19. doi: 10.2147/CIA.S302389.
Phrommintikul A, Detnuntarat P, Prasertwitayakij N, Wongcharoen W. Prevalence of atrial fibrillation in Thai elderly. J Geriatr Cardiol. 2016;13(3):270-3. doi: 10.11909/j.issn.1671-5411.2016.03.002.
Ghate SR, Biskupiak J, Ye X, Kwong WJ, Brixner DI. All-cause and bleeding-related health care costs in warfarin-treated patients with atrial fibrillation. J Manag Care Pharm. 2011;17(9):672-84. doi: 10.18553/jmcp.2011.17.9.672.
Roberts KM, Knight TB, Padilla-Tolentino E, Murthy M, Peterson EJ. Length of stay comparison between rivaroxaban and warfarin in the treatment of pulmonary embolism: results from a real-World observational cohort study. Thrombosis. 2015;2015:414523. doi: 10.1155/2015/414523.
Charlton B, Adeboyeje G, Barron JJ, Grady D, Shin J, Redberg RF. Length of hospitalization and mortality for bleeding during treatment with warfarin, dabigatran, or rivaroxaban. PLoS One. 2018;13(3):e0193912. doi: 10.1371/journal.pone.0193912.
George D, Wong CA, Thanimalai S, Tan HS. Severity and hospitalization cost related to warfarin-related adverse events in a tertiary Malaysian hospital. Hosp Pharm. 2022;57(5):633–8. doi: 10.1177/00185787211070182.
Hylek EM, Evans-Molina C, Shea C, Henault LE, Regan S. Major hemorrhage and tolerability of warfarin in the first year of therapy among elderly patients with atrial fibrillation. Circulation. 2007;115(21):2689-96. doi: 10.1161/CIRCULATIONAHA.106.653048.
Franco L, Becattini C, Beyer-Westendorf J, Vanni S, Nitti C, Re R, et al. Definition of major bleeding: prognostic classification. J Thromb Haemost. 2020;18(11):2852-60. doi: 10.1111/jth.15048.
Lan Y, Chen J, Niu P, Huang X, Dong X, You C, et al. Efficacy, safety, and bleeding risk factor analysis of oral anticoagulants in AF patients ≥ 65 years of age: a multicenter retrospective cohort study. BMC Geriatr. 2025;25(1):203. doi: 10.1186/s12877-025-05838-4.
Rydberg DM, Linder M, Malmström RE, Andersen M. Risk factors for severe bleeding events during warfarin treatment: the influence of sex, age, comorbidity, and co-medication. Eur J Clin Pharmacol. 2020;76(6):867-76. doi: 10.1007/s00228-020-02856-6.
Hicks KA, Stockbridge NL, Targum SL, Temple RJ. Bleeding Academic Research Consortium consensus report: the Food and Drug Administration perspective.Circulation. 2011;123(23):2664-5. doi: 10.1161/CIRCULATIONAHA.111.032433.
Palareti G, Hirsh J, Legnani C, Manotti C, D'Angelo A, Pengo V, et al. Oral anticoagulation treatment in the elderly: a nested, prospective, case-control study. Arch Intern Med. 2000;160(4):470-8. doi: 10.1001/archinte.160.4.470.
Priksri W, Rattanavipanon W, Saejear W, Tanyasaensook K, Phrommintikul A, Chulavatnatol S, et al. Incidence, risk factors, and outcomes of warfarin-associated major bleeding in Thai population. Pharmacoepidemiol Drug Saf. 2019;28(7):942-50. doi: 10.1002/pds.4781.
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2025 Health Administration Division, Office of the Permanent Secretary, Ministry of Public Health and The Society of Hospital Pharmacist, Ministry of Public Health

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
วารสารเภสัชกรรมคลินิกเป็นวารสารในรูปแบบเปิด ผู้ใช้ทั่วไปสามารถเข้าถึง ดาวน์โหลด เอกสารไฟล์บทความบนเว็บไซต์วารสาร โดยไม่มีค่าใช้จ่ายแต่อย่างใด
ข้อความภายในบทความที่ตีพิมพ์ในวารสารเภสัชกรรมคลินิกทั้งหมด รวมถึงรูปภาพประกอบ ตาราง เป็นลิขสิทธิ์ของกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข อนุญาตให้นำไปใช้ประโยชน์และเผยแพร่ต่อได้โดยอยู่ภายใต้เงื่อนไขสัญญาอนุญาตครีเอทีฟคอมมอนส์ โดยต้องแสดงที่มาจากวารสาร – ไม่ใช้เพื่อการค้า – ห้ามแก้ไขดัดแปลง (Creative Commons Attribution-NonCommercial-NoDerivatives 4.0; CC BY-NC-ND 4.0) การนำเนื้อหา ข้อความหรือข้อคิดเห็น รูปภาพ ตาราง ของบทความไปจัดพิมพ์เผยแพร่ในรูปแบบต่าง ๆ เพื่อใช้ประโยชน์ในเชิงพาณิชย์ ต้องได้รับอนุญาตจากกองบรรณาธิการวารสารเภสัชกรรมคลินิกอย่างเป็นลายลักษณ์อักษร
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และบุคลากรในกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้เขียน ไม่เกี่ยวข้องกับกองบรรณาธิการ
