
ปัจจัยที่มีผลต่อการควบคุมค่าทีทีอาร์ในผู้ป่วยที่ใช้ยาวาร์ฟาริน ในคลินิกวาร์ฟาริน โรงพยาบาลพังงา
คำสำคัญ:
วาร์ฟาริน, ปัจจัย, พฤติกรม, time in therapeutic range, INRบทคัดย่อ
บทคัดย่อ
ความเป็นมา: ผู้ป่วยที่ใช้วาร์ฟารินจำเป็นต้องควบคุมค่า INR ให้อยู่ในช่วงเป้าหมาย โดยใช้ระยะเวลาที่ค่า INR อยู่ในช่วงเป้าหมาย (time in therapeutic range; TTR) เป็นตัวชี้วัดคุณภาพการรักษา ทั้งนี้ มีหลายปัจจัยที่ส่งผลต่อการควบคุม TTR
วัตถุประสงค์: เพื่อศึกษาปัจจัยที่มีผลต่อการควบคุม TTR ในผู้ป่วยที่ใช้วาร์ฟาริน
วิธีวิจัย: การวิจัยเชิงวิเคราะห์แบบย้อนหลังในผู้ป่วยที่ใช้วาร์ฟาริน จำนวน 300 ราย ระหว่างมกราคม พ.ศ. 2563 – ธันวาคม พ.ศ. 2567 โดยเก็บข้อมูลจากเวชระเบียนและแบบสอบถาม 6 ส่วน ครอบคลุมข้อมูลส่วนบุคคล ปัจจัยทางชีวภาพ และปัจจัยด้านพฤติกรรม/จิตสังคม วิเคราะห์ด้วยสถิติเชิงพรรณนา univariate binary logistic regression และ multivariate binary logistic regression
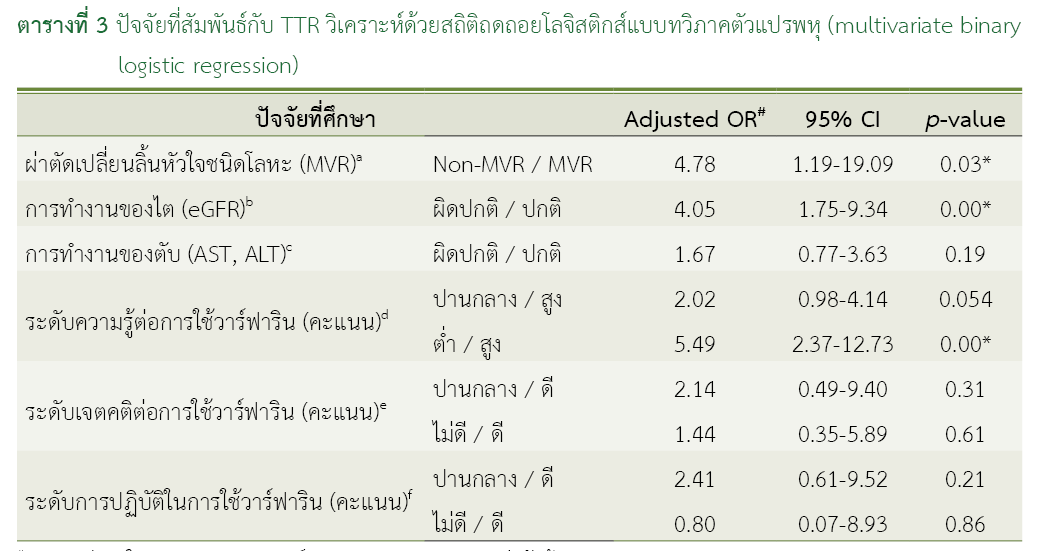
ผลการวิจัย: กลุ่มตัวอย่าง 300 คน พบว่าร้อยละ 73.67 มีการควบคุม TTR ตามเป้าหมาย การวิเคราะห์ความสัมพันธ์ทีละปัจจัยพบว่าปัจจัยที่มีความสัมพันธ์อย่างมีนัยสำคัญทางสถิติ (p-value < 0.05) ได้แก่ การทำงานของไต การทำงานของตับ การผ่าตัดเปลี่ยนลิ้นหัวใจชนิดโลหะ รวมถึงความรู้ เจตคติ และการปฏิบัติเกี่ยวกับวาร์ฟาริน เมื่อวิเคราะห์ความสัมพันธ์ของตัวแปรที่มีนัยสำคัญทางสถิติทั้งหมดร่วมกัน พบว่าการผ่าตัดเปลี่ยนลิ้นหัวใจชนิดโลหะ การทำงานของไต และความรู้เกี่ยวกับการใช้วาร์ฟาริน มีความสัมพันธ์อย่างมีนัยสำคัญทางสถิติโดยอิสระ (p-value < 0.05)
สรุปผล: ปัจจัยทางชีวภาพและปัจจัยด้านพฤติกรรม/จิตสังคม มีบทบาทสำคัญต่อการควบคุม TTR ผลการศึกษาสามารถนำไปใช้พัฒนาแนวทางการคัดกรองผู้ป่วยกลุ่มเสี่ยงและปรับปรุงการให้ความรู้ในคลินิกวาร์ฟาริน
เอกสารอ้างอิง
Schmitt L, Speckman J, Ansell J. Quality assessment of anticoagulation dose management: comparative evaluation of measures of time-in-therapeutic range. J Thromb Thrombolysis. 2003;15(3):213–6. doi: 10.1023/B:THRO.0000011377.78585.63.
Rose AJ, Hylek EM, Ozonoff A, Ash AS, Reisman JI, Berlowitz DR. Risk-adjusted percent time in therapeutic range as a quality indicator for outpatient oral anticoagulation: results of the Veterans Affairs Study to Improve Anticoagulation (VARIA). Circ Cardiovasc Qual Outcomes. 2011;4(1):22–9. doi: 10.1161/CIRCOUTCOMES.110.957738.
Feungfu L, Raksasilp T, Swaengsak N, Chysirichote T, Santiyanon N, Yeephu S. Evaluation of time in therapeutic range among patients receiving warfarin therapy: a retrospective cohort study at one private hospital in Thailand. Pharm Sci Asia. 2021;48(2):107–14. doi: 10.29090/psa.2021.02.19.143.
Absher RK, Moore ME, Parker MH. Patient-specific factors predictive of warfarin dosage requirements. Ann Pharmacother. 2002;36(10):1512–7. doi: 10.1345/aph.1C025.
Tellor KB, Nguyen SN, Bultas AC, Armbruster AL, Greenwald NA, Yancey AM. Evaluation of the impact of body mass index on warfarin requirements in hospitalized patients. Ther Adv Cardiovasc Dis. 2018;12(8):207–16. doi: 10.1177/1753944718781295.
พีระพงศ์ ภูบาล. การศึกษาสถานการณ์ปัญหาการใช้ยาวาร์ฟารินและการพัฒนาระบบการติดตามดูแลความปลอดภัยจากการใช้ยาวาร์ฟารินในระดับปฐมภูมิ [วิทยานิพนธ์, อินเทอร์เน็ต]. มหาสารคาม: มหาวิทยาลัยมหาสารคาม; 2563 [สืบค้นเมื่อ 15 ก.ค. 2568]. สืบค้นจาก: http://202.28.34.124/dspace/handle/123456789/940
อภิชัย มาสุขใจ. การศึกษาทดสอบความถูกต้องของปัจจัยที่ใช้พยากรณ์การใช้ยาวาร์ฟารินที่ไม่ได้ประสิทธิภาพในคนไทยที่มีภาวะ หัวใจห้องบนเต้นผิดจังหวะแบบสั่นระริกที่ไม่ได้เกิดจากลิ้นหัวใจผิดปกติ [วิทยานิพนธ์, อินเทอร์เน็ต]. กรุงเทพมหานคร: คณะแพทยศาสตร์ จุฬาลงกรณ์มหาวิทยาลัย; 2565 [สืบค้นเมื่อ 15 ก.ค. 2568]. สืบค้นจาก: https://digital.car.chula.ac.th/chulaetd/6747/
Batra G, Modica A, Renlund H, Larsson A, Christersson C, Held C. Oral anticoagulants, time in therapeutic range and renal function over time in real-life patients with atrial fibrillation and chronic kidney disease. Open Heart. 2022;9(2):e002043. doi: 10.1136/openhrt-2022-002043.
Gish RG, Flamm SL. Anticoagulation in patients with chronic liver disease. Gastroenterol Hepatol. 2021;17(1 Suppl 1):10–5. PMID: 34135699.
Zhu X, Xiao X, Wang S, Chen X, Lu G, Li X. Rosendaal linear interpolation method appraising of time in therapeutic range in patients with 12-week follow-up interval after mechanical heart valve replacement. Front Cardiovasc Med. 2022;9:925571. doi: 10.3389/fcvm.2022.925571.
มันติวีร์ นิ่มวรพันธ์. ปัจจัยที่มีผลต่อการควบคุมค่าการแข็งตัวของเลือดในผู้ป่วยนอกที่ได้รับการรักษาด้วยยาวาร์ฟาริน โรงพยาบาลมหาราชนครเชียงใหม่ [วิทยานิพนธ์, อินเทอร์เน็ต]. เชียงใหม่: มหาวิทยาลัยเชียงใหม่; 2550 [สืบค้นเมื่อ 15 ก.ค. 2568]. สืบค้นจาก: https://cmudc.library.cmu.ac.th/frontend/Info/item/dc:107613
Sridharan K, Al Banna R, Qader AM, Husain A. Does fasting during Ramadan influence the therapeutic effect of warfarin? J Clin Pharm Ther. 2021;46(1):86–92. doi: 10.1111/jcpt.13254.
นพดล กิตติถาวร. การพัฒนางานบริบาลทางเภสัชกรรมในคลินิกวาร์ฟารินของผู้ป่วยในโรงพยาบาลปลาปาก. วารสารโรงพยาบาลนครพนม [อินเทอร์เน็ต]. 2567 [สืบค้นเมื่อ 15 ก.ค. 2568];11(1):e267977. สืบค้นจาก: https://he01.tci-thaijo.org/index.php/nkpjournal_9/issue/view/17904
Praxedes MFDS, Silva JLPD, Cruz AJAD, Viana CC, Barbosa HC, Guimarães NS, Martins MAP. Assessment of the relationship between the level of patient knowledge on warfarin therapy and the quality of oral anticoagulation: a systematic review and meta-analysis. PLoS ONE. 2023;18(8):e0289836. doi: 10.1371/journal.pone.0289836.
จันทร์ชุดากร จันทร์อำพล, ฉวีวรรณ บุญสุยา, คัติยา อีวาโนวิช. การกินยาวาร์ฟารินตามคำสั่งแพทย์อย่างเคร่งครัดของผู้ป่วยโรคหัวใจและหลอดเลือด โรงพยาบาลพระนารายณ์มหาราช จังหวัดลพบุรี. วารสารการแพทย์และสาธารณสุขเขต 4 [อินเทอร์เน็ต]. 2566 [สืบค้นเมื่อ 12 มิ.ย. 2568];13(3):59-70. สืบค้นจาก: https://he01.tci-thaijo.org/index.php/JMPH4/article/view/262715
Kilic S, Çelik A, Seyis AS, Kurmus O, Tülüce K, Emren ZY, et al. Potential factors affecting the anticoagulation control in patients treated with warfarin: Results WARFARIN‑TR study. Int J Cardiovasc Acad. 2018;4(4):86–9. doi: 10.4103/IJCA.IJCA_43_18.
Robles-Diaz M, Lucena MI, Kaplowitz N, Stephens C, Medina-Cáliz I, González-Jimenez A, et al. Use of Hy's law and a new composite algorithm to predict acute liver failure in patients with drug-induced liver injury. Gastroenterology. 2014;147(1):109–18.e5. doi: 10.1053/j.gastro.2014.03.050.
Farrington K, Covic A, Nistor I, Aucella F, Clyne N, De Vos L, et al. Clinical practice guideline on management of older patients with chronic kidney disease stage 3b or higher (eGFR <45 mL/min/1.73 m²): a summary document from the European Renal Best Practice Group. Nephrol Dial Transplant. 2017;32(1):9–16. doi: 10.1093/ndt/gfw411.
Ngamjarus C, Pattanittum P. n4Studies: application for sample size calculation in health science research. Version 2.3 [Internet]. n.p: Apple Inc.; 2024 [cited 2025 Apr 15] Avaible from: App store
Bloom BS. Learning for mastery [Internet]. Los Angeles: Center for the Study of Evaluation of Instructional Programs, University of California; 1968 [cited 2025 Jul 15]. Available from: https://files.eric.ed.gov/fulltext/ED053419.pdf
Reiffel JA. Time in the therapeutic range (TTR): an overly simplified conundrum. J Innov Cardiac Rhythm Manag. 2017;8(3):2643–6. doi: 10.19102/icrm.2017.080302.
อรชร สุนทรารักษ์. การพัฒนาระบบการดูแลผู้ป่วยที่ได้รับยาวาร์ฟารินแบบสหวิชาชีพ โดยใช้แนวคิดการจัดการตนเองร่วมกับการจัดการรายกรณี โรงพยาบาลนาหว้า จังหวัดนครพนม. วารสารการพยาบาลและวิทยาศาสตร์สุขภาพ มหาวิทยาลัยนครพนม [อินเทอร์เน็ต]. 2566 [สืบค้นเมื่อ 11 ก.ค. 2568];1(2):63–73. สืบค้นจาก: https://he03.tci-thaijo.org/index.php/bcnnjournal/article/view/1825
Viana CC, Praxedes MFdS, Abreu MHNGd, Sousa WJFNd, Ferreira CRL, Campos EIdF, et al. Quality of oral anticoagulation control with warfarin according to sex: a cross-sectional study. Int J Environ Res Public Health. 2025;22(1):65. doi: 10.3390/ijerph22010065.
ดาวน์โหลด
เผยแพร่แล้ว
วิธีการอ้างอิง
ฉบับ
บท
การอนุญาต
ลิขสิทธิ์ (c) 2025 กองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
วารสารเภสัชกรรมคลินิกเป็นวารสารในรูปแบบเปิด ผู้ใช้ทั่วไปสามารถเข้าถึง ดาวน์โหลด เอกสารไฟล์บทความบนเว็บไซต์วารสาร โดยไม่มีค่าใช้จ่ายแต่อย่างใด
ข้อความภายในบทความที่ตีพิมพ์ในวารสารเภสัชกรรมคลินิกทั้งหมด รวมถึงรูปภาพประกอบ ตาราง เป็นลิขสิทธิ์ของกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข อนุญาตให้นำไปใช้ประโยชน์และเผยแพร่ต่อได้โดยอยู่ภายใต้เงื่อนไขสัญญาอนุญาตครีเอทีฟคอมมอนส์ โดยต้องแสดงที่มาจากวารสาร – ไม่ใช้เพื่อการค้า – ห้ามแก้ไขดัดแปลง (Creative Commons Attribution-NonCommercial-NoDerivatives 4.0; CC BY-NC-ND 4.0) การนำเนื้อหา ข้อความหรือข้อคิดเห็น รูปภาพ ตาราง ของบทความไปจัดพิมพ์เผยแพร่ในรูปแบบต่าง ๆ เพื่อใช้ประโยชน์ในเชิงพาณิชย์ ต้องได้รับอนุญาตจากกองบรรณาธิการวารสารเภสัชกรรมคลินิกอย่างเป็นลายลักษณ์อักษร
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และบุคลากรในกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้เขียน ไม่เกี่ยวข้องกับกองบรรณาธิการ
