
การศึกษาประสิทธิผลของการทดแทนอัลบูมินในผู้ป่วยที่ใช้เครื่องช่วยหายใจและมีภาวะอัลบูมินในเลือดต่ำ โรงพยาบาลแพร่
คำสำคัญ:
ภาวะอัลบูมินในเลือดต่ำ, ช็อกจากการติดเชื้อ, ปอดบวม, ทางเดินหายใจล้มเหลวเฉียบพลัน, สารเพิ่มปริมาตรน้ำในหลอดเลือดอัลบูมินบทคัดย่อ
ความเป็นมา: ภาวะอัลบูมินในเลือดต่ำนำไปสู่ภาวะทางเดินหายใจล้มเหลวเฉียบพลันและการเสียชีวิต การใช้อัลบูมินเป็นสารเพิ่มปริมาตรน้ำในหลอดเลือดในผู้ป่วยวิกฤติที่ใช้เครื่องช่วยหายใจมีหลักฐานที่ยังหาข้อสรุปไม่ชัดเจน
วัตถุประสงค์: ศึกษาความสัมพันธ์ของอัตราการเสียชีวิตภายใน 28 วัน ระยะเวลาไม่ใช้เครื่องช่วยหายใจภายใน 28 วัน และระยะเวลาการนอนโรงพยาบาลของผู้ป่วยที่ใช้เครื่องช่วยหายใจที่มีภาวะอัลบูมินในเลือดต่ำเปรียบเทียบผู้ป่วยที่ได้รับอัลบูมินทดแทนและไม่ได้รับอัลบูมิน
วิธีวิจัย: การศึกษาย้อนหลังในผู้ป่วย 443 รายที่ใช้เครื่องช่วยหายใจจากภาวะช็อกจากการติดเชื้อหรือโรคปอดบวมหรือทางเดินหายใจล้มเหลวเฉียบพลันและมีภาวะอัลบูมินในเลือดต่ำ (<2.5 g/dL) แบ่งเป็นกลุ่มได้รับอัลบูมิน 20% และไม่ได้รับอัลบูมิน วิเคราะห์ผลลัพธ์หลักด้วย modified Poisson พร้อม robust SE เพื่อประมาณ RR (95% CI) เลือกตัวแปรร่วมจากการถดถอยโลจิสติกแบบตัวแปรเดียว (p-value < 0.05) และ DAGs ทดสอบปฏิสัมพันธ์และประเมินพหุสหสัมพันธ์ (VIF < 5) ผลลัพธ์รองเปรียบเทียบด้วย t-test หรือ Wilcoxon rank sum test
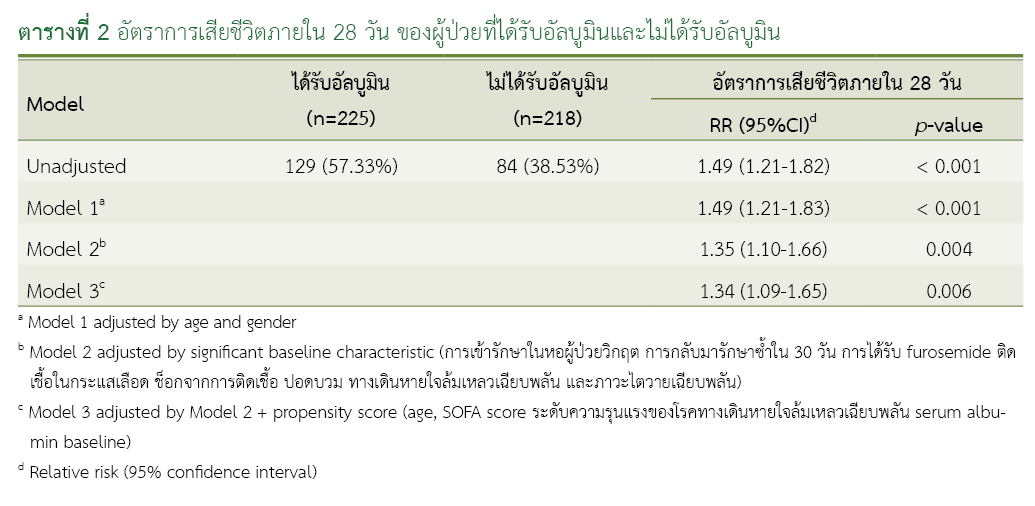
ผลการวิจัย: กลุ่มได้รับอัลบูมินเสียชีวิตภายใน 28 วัน 129 รายจาก 225 ราย (ร้อยละ 57.33) กลุ่มไม่ได้รับอัลบูมินเสียชีวิต 84 รายจาก 218 ราย (ร้อยละ 38.53) (RR = 1.34; 95% CI: 1.09-1.65, p-value = 0.006) ผู้ป่วยที่มีอัลบูมินพื้นฐาน < 1.5 g/dL หรือ 1.6-2.0 g/dL หรือ SOFA ≥ 6 มีอัตราการเสียชีวิตไม่แตกต่างกันอย่างมีนัยสำคัญทางสถิติ แต่การได้รับอัลบูมินในผู้ป่วยอายุ < 40 ปี อัตราการเสียชีวิตลดลงอย่างมีนัยสำคัญทางสถิติ ผลลัพธ์รองกลุ่มที่ได้รับอัลบูมินมีระยะเวลาที่ไม่ใช้เครื่องช่วยหายใจภายใน 28 วันที่สั้นกว่า (p-value < 0.001) และระยะเวลานอนโรงพยาบาลนานกว่ากลุ่มที่ไม่ใช้อัลบูมินอย่างมีนัยสำคัญทางสถิติ (p-value < 0.001)
สรุปผลการวิจัย: ผู้ป่วยที่ใช้เครื่องช่วยหายใจจากภาวะช็อกจากการติดเชื้อหรือปอดบวมหรือทางเดินหายใจล้มเหลวเฉียบพลันและมีระดับอัลบูมินในเลือดต่ำ (<2.5 g/dL) การได้รับอัลบูมินไม่ได้เพิ่มอัตราการรอดชีวิตภายใน 28 วันเปรียบเทียบกับการไม่ได้รับอัลบูมิน
เอกสารอ้างอิง
Gibbs J, Cull W, Henderson W, Daley J, Hur K, Khuri SF. Preoperative serum albumin level as a predictor of operative mortality and morbidity: results from the National VA Surgical Risk Study. Arch Surg. 1999;134(1):36-42. doi: 10.1001/archsurg.134.1.36.
McNeil JB, Jackson KE, Wang C, Siew ED, Vincz AJ, Shaver CM, et al. Linear association between hypoalbuminemia and increased risk of acute respiratory distress syndrome in critically ill adults. Crit Care Explor. 2021;3(9):e0527. doi: 10.1097/CCE.0000000000000527.
Alexander MR, Stumpf JL, Nostrant TT, Khanderia U, Eckhauser FE, Colvin CL. Albumin utilization in a university hospital. DICP. 1989;23(3):214-7. doi: 10.1177/106002808902300304.
Tarín Remohí MJ, Sánchez Arcos A, Santos Ramos B, Bautista Paloma J, Guerrero Aznar MD. Costs related to inappropriate use of albumin in Spain. Ann Pharmacother. 2000;34(10):1198-205. doi: 10.1345/aph.19385.
Debrix I, Combeau D, Stephan F, Benomar A, Becker A. Clinical practice guidelines for the use of albumin: results of a drug use evaluation in a Paris hospital. Tenon Hospital Paris. Pharm World Sci. 1999;21(1):11-6. doi: 10.1023/a:1008635005398.
Cochrane Injuries Group Albumin Reviewers. Human albumin administration in critically ill patients: systematic review of randomised controlled trials. BMJ. 1998;317(7153):235-40. doi: 10.1136/bmj.317.7153.235.
Wilkes MM, Navickis RJ. Patient survival after human albumin administration: a meta-analysis of randomized controlled trials. Ann Intern Med. 2001;135(3):149-64. doi:10.7326/0003-4819-135-3-200108070-00007.
Foley EF, Borlase BC, Dzik WH, Bistrian BR, Benotti PN. Albumin supplementation in the critically ill: a prospective, randomized trial. Arch Surg. 1990;125(6):739-42. doi: 10.1001/archsurg.1990.01410180063012.
Tseng CH, Chen TT, Wu MY, Chan MC, Shih MC, Tu YK. Resuscitation fluid types in sepsis, surgical, and trauma patients: a systematic review and sequential network meta-analyses. Crit Care. 2020;24(1):693. doi: 10.1186/s13054-020-03419-y.
Wang X, Zhang T, Gao X, Cai H, Guo M, Liu Q, et al. Early human albumin administration is associated with reduced mortality in septic shock patients with acute respiratory distress syndrome: a retrospective study from the MIMIC-III database. Front Physiol. 2023;14:1142329. doi: 10.3389/fphys.2023.1142329.
Annane D, Siami S, Jaber S, Martin C, Elatrous S, Descorps Declère A, et al. Effects of fluid resuscitation with colloids vs crystalloids on mortality in critically ill patients presenting with hypovolemic shock: the CRISTAL randomized trial. JAMA. 2013;310(17):1809-17. doi: 10.1001/jama.2013.280502.
Caironi P, Tognoni G, Masson S, Fumagalli R, Pesenti A, Romero M, et al. Albumin replacement in patients with severe sepsis or septic shock. N Engl J Med. 2014;370(15):1412-21. doi: 10.1056/NEJMoa1305727.
ดาวน์โหลด
เผยแพร่แล้ว
วิธีการอ้างอิง
ฉบับ
บท
การอนุญาต
ลิขสิทธิ์ (c) 2025 กองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
วารสารเภสัชกรรมคลินิกเป็นวารสารในรูปแบบเปิด ผู้ใช้ทั่วไปสามารถเข้าถึง ดาวน์โหลด เอกสารไฟล์บทความบนเว็บไซต์วารสาร โดยไม่มีค่าใช้จ่ายแต่อย่างใด
ข้อความภายในบทความที่ตีพิมพ์ในวารสารเภสัชกรรมคลินิกทั้งหมด รวมถึงรูปภาพประกอบ ตาราง เป็นลิขสิทธิ์ของกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข อนุญาตให้นำไปใช้ประโยชน์และเผยแพร่ต่อได้โดยอยู่ภายใต้เงื่อนไขสัญญาอนุญาตครีเอทีฟคอมมอนส์ โดยต้องแสดงที่มาจากวารสาร – ไม่ใช้เพื่อการค้า – ห้ามแก้ไขดัดแปลง (Creative Commons Attribution-NonCommercial-NoDerivatives 4.0; CC BY-NC-ND 4.0) การนำเนื้อหา ข้อความหรือข้อคิดเห็น รูปภาพ ตาราง ของบทความไปจัดพิมพ์เผยแพร่ในรูปแบบต่าง ๆ เพื่อใช้ประโยชน์ในเชิงพาณิชย์ ต้องได้รับอนุญาตจากกองบรรณาธิการวารสารเภสัชกรรมคลินิกอย่างเป็นลายลักษณ์อักษร
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และบุคลากรในกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้เขียน ไม่เกี่ยวข้องกับกองบรรณาธิการ
