Effectiveness of Developing a Centralized Sterile Drug Preparation System for Individual Patients in a Tertiary Hospital
Keywords:
sterile drug preparation, individual patients, centralized system, tertiary hospitalAbstract
Background: Preparing sterile medications for individual patients in tertiary hospitals requires effective management. Previous operations identified issues related to drug safety and quality. Therefore, the Pharmacy Division developed a centralized sterile medication preparation system for individual patients.
Objectives: To examine the existing situation, system development process, and effectiveness of a centralized sterile medication preparation system for individual patients in a tertiary hospital.
Methods: This research and development study utilized retrospective data and was conducted in three stages: (1) analyzing the problem situation using retrospective data from fiscal years 2019–2024; (2) developing and implementing a centralized drug preparation system in conjunction with a newly developed computer program; and (3) evaluating the effectiveness of the developed system by comparing outcomes before implementation (fiscal year 2021) and after implementation (fiscal year 2024), focusing on drug waiting time, cost, and medication errors. Data were analyzed using descriptive statistics, inferential statistics, and content analysis.
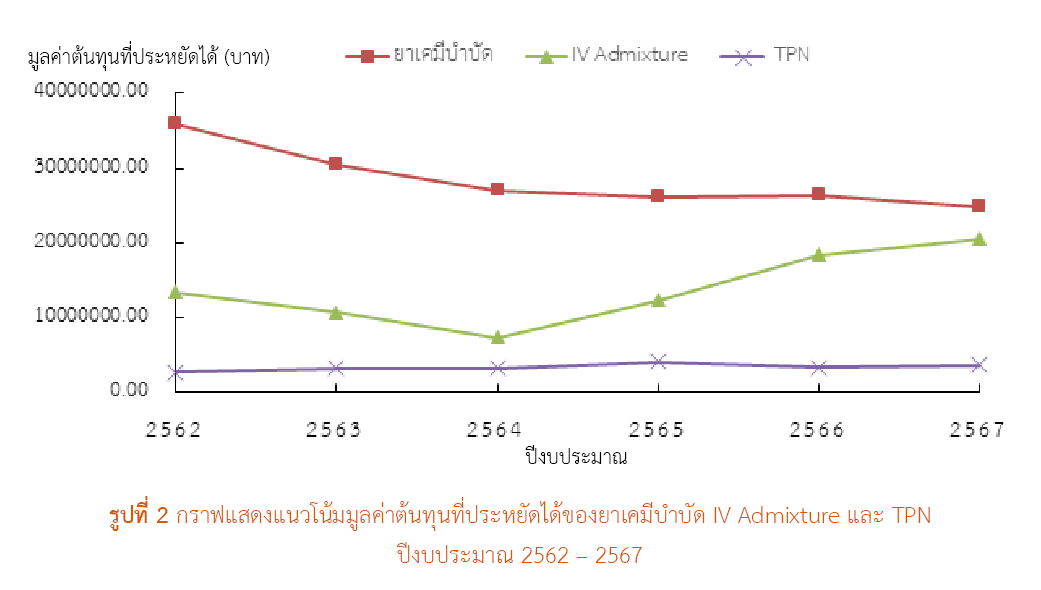
Results: (1) Situation and Problems: The drug preparation process was complex, unsystematic, and lacked data connectivity. (2) System Development: A centralized sterile drug preparation system was developed, incorporating automated dose calculation, alert notifications, and centralized data storage. (3) System Effectiveness: (a) Waiting time significantly decreased after system implementation. Chemotherapy preparation time decreased by 48.95 minutes (56.4%), and intravenous nutrition preparation time decreased by 6.24 minutes (46.3%), with statistical significance at p-value < 0.001. (b) The average annual cost savings were 28.50 million baht for chemotherapy drugs, 13.84 million baht for IV admixtures, and 3.45 million baht for total parenteral nutrition (TPN). (c) Prescribing errors were reduced by 18.78% for chemotherapy drugs, 32.35% for IV admixtures, and 22.79% for TPN, with statistically significant differences at p-value < 0.05.
Conclusion: The developed system represents an innovative approach that significantly improves the quality of drug management within the hospital by reducing errors and increasing operational efficiency. It also strengthens operational standards in alignment with international principles.
References
กฤษณ์ สุขนันทร์ธะ, เปญจมาภรณ์ อภิรมย์รักษ์. แนวทางการผลิตยาเตรียมปราศจากเชื้อในโรงพยาบาลตาม ASHP guidelines on compounding sterile preparations [อินเทอร์เน็ต]. นนทบุรี: ศูนย์การศึกษาต่อเนื่องทางเภสัชศาสตร์ สภาเภสัชกรรม; 2560 [สืบค้นเมื่อ 30 มี.ค. 2567]. สืบค้นจาก: https://ccpe.pharmacycouncil.org/index.php?option=article_detail&subpage=article_detail&id=411
ธนิต วิริยะธารากิจ. คู่มือการปฏิบัติงานการเตรียมยาฉีดปราศจากเชื้อ [อินเทอร์เน็ต]. กรุงเทพมหานคร: งานผลิตยา ฝ่ายเภสัชกรรม คณะแพทยศาสตร์โรงพยาบาลรามาธิบดี มหาวิทยาลัยมหิดล; 2567 [สืบค้นเมื่อ 30 มี.ค. 2567]. สืบค้นจาก: https://repository.li.mahidol.ac.th/handle/123456789/109683
รัตติกรณ์ บุญพัฒน์, รัศมี ลีประไพวงษ์, สุภัทรา ปุญญนิรันดร์, ชญานี อิสรไกรศีล, กันตพัฒน์ ตันธนาวุฒิวัฒน์. โครงการการพัฒนาระบบบริหารจัดการยาปราศจากเชื้อในห้องยา หู ตา คอ และจมูก คณะแพทยศาสตร์ศิริราชพยาบาล. เวชบันทึกศิริราช [อินเทอร์เน็ต]. 2563 [สืบค้นเมื่อ 30 ก.ย. 2568];13(2):85-95. สืบค้นจาก: https://he02.tci-thaijo.org/index.php/simedbull/article/view/241653
สถาบันรับรองคุณภาพสถานพยาบาล (องค์กรมหาชน). M1.1 safe from high alert drug. ใน: เป้าหมายความปลอดภัยของผู้ป่วยของประเทศไทย พ.ศ. 2561. นนทบุรี: สถาบันรับรองคุณภาพสถานพยาบาล (องค์กรมหาชน); 2561.
สุนทร ปภานิธินันท. แนวคิดการจัดการยาที่มีความเสี่ยงสูง (high alert drug : HAD) เพื่อความปลอดภัยในโรงพยาบาล [อินเทอร์เน็ต]. นนทบุรี: ศูนย์การศึกษาต่อเนื่องทางเภสัชศาสตร์ สภาเภสัชกรรม; 2563 [สืบค้นเมื่อ 30 มี.ค. 2567]. สืบค้นจาก: https://ccpe.pharmacycouncil.org/index.php?option=article_detail&subpage=article_detail&id=834
ถิรพิทย์ สุบงกช. สถานที่และการควบคุมสภาวะแวดล้อมสำหรับการผลิตยาปราศจาศจากเชื้อ [อินเทอร์เน็ต]. นนทบุรี: ศูนย์การศึกษาต่อเนื่องทางเภสัชศาสตร์ สภาเภสัชกรรม; 2560 [สืบค้นเมื่อ 30 มี.ค. 2567]. สืบค้นจาก: http://www.ccpe.pharmacycouncil.org/index.php?option=article_detail&subpage=article_detail&id=405
American Society of Health-System Pharmacists. ASHP guidelines on compounding sterile preparations. Am J Health-Syst Pharm. 2014;71(2):145-66. doi: 10.2146/sp140001.
Poon EG, Keohane CA, Yoon CS, Ditmore M, Bane A, Levtzion-Korach O, et al. Effect of bar-code technology on the safety of medication administration. N Engl J Med. 2010;362(18):1698-707. doi: 10.1056/NEJMsa0907115.
Pedersen CA, Schneider PJ, Ganio MC, Scheckelhoff DJ. ASHP national survey of pharmacy practice in hospital settings: dispensing and administration-2020. Am J Health Syst Pharm. 2021;78(12):1074-93. doi: 10.1093/ajhp/zxab120.
Jessurun JG, Hunfeld NGM, van Rosmalen J, van Dijk M, van den Bemt PMLA. Effect of a pharmacy-based centralized intravenous admixture service on the prevalence of medication errors: a before-and-after study. J Patient Saf. 2022;18(8):e1181-8. doi: 10.1097/PTS.0000000000001047.
Institute for Safe Medication Practices (ISPM). ISMP releases top 10 list of medication errors and hazards in 2020. React Wkly. 2021;1844:7. doi: 10.1007/s40278-021-91454-9.
Phueanpinit P, Pongwecharak J, Krska J, Jarernsiripornkul N. Evaluation of community pharmacists' roles in screening and communication of risks about non-steroidal anti-inflammatory drugs in Thailand. Prim Health Care Res Dev. 2018;19(6):598-604. doi: 10.1017/S1463423618000142.
Larrouturou P, Rebischung JL, Taugourdeau MC, Sauvaget J, Huchet J. Comparison of costs linked to the preparation and administration of fluorouracil as a continuous infusion based on three techniques. Pharm Weekbl Sci. 1992;14(6):357–9. doi: 10.1007/BF01970172.
Nurgat Z, Faris D, Mominah M, Vibar A, Al-Jazairi A, Ewing S, et al. A three-year study of a first-generation chemotherapy-compounding robot. Am J Health Syst Pharm. 2015;72(12):1036-45. doi: 10.2146/ajhp140256.
สมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย). กรอบงานพื้นฐานระบบยา [อินเทอร์เน็ต]. กรุงเทพมหานคร: สมาคมเภสัชกรรมโรงพยาบาล (ประเทศไทย); 2563 [สืบค้นเมื่อ 30 มี.ค. 2567]. สืบค้นจาก: https://www.thaihp.org/wp-content/uploads/2022/06/หนังสือกรอบงานพื้นฐาน.pdf
Downloads
Published
How to Cite
Issue
Section
License
Copyright (c) 2026 Health Administration Division, Office of the Permanent Secretary, Ministry of Public Health and The Society of Hospital Pharmacist, Ministry of Public Health

This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivatives 4.0 International License.
วารสารเภสัชกรรมคลินิกเป็นวารสารในรูปแบบเปิด ผู้ใช้ทั่วไปสามารถเข้าถึง ดาวน์โหลด เอกสารไฟล์บทความบนเว็บไซต์วารสาร โดยไม่มีค่าใช้จ่ายแต่อย่างใด
ข้อความภายในบทความที่ตีพิมพ์ในวารสารเภสัชกรรมคลินิกทั้งหมด รวมถึงรูปภาพประกอบ ตาราง เป็นลิขสิทธิ์ของกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และ ชมรมเภสัชกรโรงพยาบาลกระทรวงสาธารณสุข อนุญาตให้นำไปใช้ประโยชน์และเผยแพร่ต่อได้โดยอยู่ภายใต้เงื่อนไขสัญญาอนุญาตครีเอทีฟคอมมอนส์ โดยต้องแสดงที่มาจากวารสาร – ไม่ใช้เพื่อการค้า – ห้ามแก้ไขดัดแปลง (Creative Commons Attribution-NonCommercial-NoDerivatives 4.0; CC BY-NC-ND 4.0) การนำเนื้อหา ข้อความหรือข้อคิดเห็น รูปภาพ ตาราง ของบทความไปจัดพิมพ์เผยแพร่ในรูปแบบต่าง ๆ เพื่อใช้ประโยชน์ในเชิงพาณิชย์ ต้องได้รับอนุญาตจากกองบรรณาธิการวารสารเภสัชกรรมคลินิกอย่างเป็นลายลักษณ์อักษร
ข้อความที่ปรากฏในบทความในวารสารเป็นความคิดเห็นส่วนตัวของผู้เขียนแต่ละท่านไม่เกี่ยวข้องกับกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข และบุคลากรในกองบริหารการสาธารณสุข สำนักงานปลัดกระทรวงสาธารณสุข แต่อย่างใด ความรับผิดชอบองค์ประกอบทั้งหมดของบทความแต่ละเรื่องเป็นของผู้เขียนแต่ละท่าน หากมีความผิดพลาดใด ๆ ผู้เขียนแต่ละท่านจะรับผิดชอบบทความของตนเอง ตลอดจนความรับผิดชอบด้านเนื้อหาและการตรวจร่างบทความเป็นของผู้เขียน ไม่เกี่ยวข้องกับกองบรรณาธิการ
